FORCED IONIZATION OF IN-DOOR AIR AS AN ADJUVANT ALTERNATIVE IN THE THERAPY OF ASTHMA AND CHRONIC BRONCHITIS
Prof.dr. V Tudorache*, St. Mihaicuta*, Rodica Potre*, Anca Kigyosi**
*The Clinic of Pneumophtisiology; ** the Chair of Medical Informatics – U.M.F Timisoara
SUMMARY
Goal: The estimation of the impact of forced ionization (NaCl) of in-door air, as an adjuvant therapy of chronic bronchitis and asthma, using a device manufactured in Romania.
Protocol: a controlled placebo study for a period of 12 month. Location: patients registered in the outpatient clinic of pulmonary diseases and from a GP consulting room.
Participants: 30 patients (9F and 21 M) suffering from simple chronic bronchitis (11) and bronchial asthma (19) associated with allergic rhinitis .The patients were distributed in 2 lots, Lot I (the study), including 17 patients, and Lot II (the placebo), including the other 13 patients ,with a comparable distribution per age, pathological profile and standard treatment.
Measured variables:the basic spirometric parameters (FEV1, FVC), the number of recurrences, the necessity of a symptomatic medication, the indices of living quality.
Results: in the control lot there were noticed a minimum improvement of FEV1 (increase of 11%) the improvement of the clinical scores (diminution of cough, sputum volume, nasal congestion, ocular pruritus and so on). The effects of these modifications were an improvement of the living quality, more rare hospitalizations and a diminution of the symptomatic medication.
Conclusions: as an ancillary treatment, the forced ionization of in-door air, though it does not improve significantly the pulmonary function, improves, however, the quality of the patients` life and diminishes the rate of annual hospitalizations. It is worth being mentioned the method advantages: there is no risk, is cheap and adapted to the living space.
INTRODUCTION
The increase of morbidity of the persons suffering from an inflammatory disease of the lung, as asthma or bronchitis, is associated with the increase of air pollution with particles. As a hypothesis it is supposed that the inhaled airborne particles can amplify the inflammation of the breathing way present in these diseases, worsening the simptomatology . But the penetrabilityof an inhaled agent depends on its type (aerosol, dry powder), characteristics (concentration/tonicity, aerodynamic diameter), aerosol using conditions (ultrasonic nebulizer, or with IPP and so on), as well as on the bronchial obstruction degree when the aerosol is inhaled (Barry P., Fouroux B-2000). Given these considerations, in the attempt to heal the airways, various devices (MDI, diskhalers, turbohalers) and substances (broncho-dilator and anti-inflammatory, culminating with corticoids)
( Boe J, Dennis J -2000) were efficiently used. But the high price of these drugs and the handling of the inhaling devices, raised for discussion the adjuvant alternatives by which physiologic (normotonic solution of NaCl) or pharmacologic (magnesium sulphate, manithol, furosemide) agents, cheap and simply to be administered (speleotherapy, inhaling from nebulizers, with or without a mask, simple spray, and so on) were used for the same goals: the diminishing of inflammation and bronchial hyperreactivity, the restoring of muco-cilliary clearance and so on) ( Kugelman A, Durand M – 1997). Starting from the indisputable benefits of speleotherapy (using of the salt mines in the treatment of the obstructive bronchial syndromes), it has been looked for the creation of some microclimates simulating the conditions in a mine. Our study can be included in this last category, where the salt from a mine is placed in a device which spreads it in the environment.
MATERIAL AND METHOD
The study goal was the estimation of the impact of the forced ionization of in-door air, by using of a device developed in Romania: SALIN produced by Tehno Bionic S.R.L. Buzau.
The device working principle consists in the forced air passing through some plates with sediment layers of micro crystallized salt, which modifies the air composition and quality due to the salt sublimation.
Participants: 30 patients (9F and 21 M) suffering from simple chronic bronchitis (11) and bronchial asthma (19) associated with allergic rhinitis. The patients were distributed in 2 lots, Lot I (the study), including 17 patients, and Lot II (the control placebo), including 13 patients, divided per age and comparable pathological profile (table I). For Lot I, the air ionization was associated with the standard treatment and was carried out in the living room or in the bedroom, and for the Lot II , the device worked without the salt plates in it , the patients being treated only conventionally ( the controlled placebo study).
Only patients suffering from asthma, the 2nd – 3rd stage, were included. We proceeded to such a selection to limit the errors which can be induced by the intensely fluctuating feature of the intermittent or mild stage (the Ist one), and by underestimationscaused by the phenomenon of clinical tolerance occurring more frequently in the 4th – 5th stages. These were the reasons why only the patients suffering from bronchitis, the IInd stage (according to the international classification from Stocholm – 1999) were included, namely with simple chronic bronchitis, with a moderate pulmonary dysfunction (FEV1>50%) without any other diseases, malnutrition, or chronic use of steroids, without bronchial colonization with intensely pathogenic germs (Enterobacteriaceae, Ps aeruginosa) and frequent exacerbations (table I).
Localization: patients registered in the outpatient clinic of pulmonary diseases and from a CP consulting room.
The study protocol: a physician specialized in pulmonary diseases diagnosed and monitored. The usual control was made every 2 months (with the exception of spirometry which was performed at the beginning and after 6 and 12 months) and any time the patients or the general practitioner required. The study was carried out for 12 months.
The device was placed next to the patient’s bed, not farther than 1m, with the exhalation window directed towards the patient level. The device operated for minimum 8-10 hours /day at the last level (12) and at the last but one level (9) of intensity, at least during the night; the door and the windows of the room were closed with the view to increase as much as possible the concentration of Na aerosols. Every 3-4 months the set of plates inside the device was changed!!!(inclusively to the placebo lot).
The observation period of 12 months enabled us to appreciate more accurate the recurrences, as both diseases, but especially asthma are known as having a significant fluctuating evolution , modulated by various factors: exposure to antigens, season, atmospheric pollution, vaccinal status, and so on.
Measured variables: the basal spirometric parameters (FEV1, FVC), PEF, the number of recurrences, the demand for symptomatic medication, the indices of living quality.
A questionnaire for the clinic score estimation was used – the bronchial obstruction, the signs of rhinitis ,- adapted from Elisabeth Juniper(Juniper E, O’Byrne P et al., 1999 şi 2000). (table II).
To establish the scores and for classification in different stages during the first month , the clinical parameters were exclusively studied ,and during the last week of the first month, the specific anti-asthma/ bronchitis treatment was interrupted the clinical examination being doubled by the functional one, by associating the PEF- metry, PEF value was related .
These variables were analyzed in the beginning and the clinical-functional study was performed every 2 months, and was focused on the estimation of clinic scores, the demand for β2 – agonists, the pulmonary function (PEF+ FEV1), the annual recurrences.
The patients received the standard treatment according to the disease gravity,in case of asthma,and the conventional one in case of chronic bronchitis; including the vaccinations (anti-flu and anti-pneumococivc),too.
Results
The procedure is well tolerated, only 3 patients mentioning the noise of the device; though slightly unpleasant, nobody renounced to the treatment. The device can be handled easily and is extremely cheap; the plates were replaced twice/year and the electric power consumption was insignificant.
Among the symptoms, noticed both at asthmatic patients and at those suffering from bronchitis, the cough was the more frequent: 74%, 84% respectively. The cough, predominant in the morning, was irritating at the asthmatic patients or often productive at the bronchitis patients. Nocturnal awakenings were more frequently met at the asthmatic patients (48%). Dyspnea was present at 61% and the wheezing and the effort limitation at 48%of the patients. The calculation of the average clinical score is more relevant than the symptoms frequency, corresponding better to the severity degree in accordance with the GINA classification.
By examining the dynamic of symptomatology in the lot with asthmatic patients, a significant improvement of the scores regarding the symptoms in the morning (figure1), the nocturnal awakenings (figure 2) and of the symptomatology relating to the allergic rhinitis (figure 3) can be noticed: with reference to the lot of the patients with bronchitis, only the dypnoea showed a significant improvement (figure 4).
For the other scores the changes were not significant. As the score estimation at the moment T12 was only a snapshot, it seemed more appropriate to us to compare the scores in the beginning of the study with the medians of the intermediary scores, so that T12 in the respective figures represents the median line of the values T4-T12.
Bronchial asthma-Symptoms in the morning Bronchial asthma
Comparisons between the moments T0 and T12

Figure 1
Bronchial asthma - Nocturnal awakenings
Comparisons between the moments T0 and T12

Figure 2
Bronchial asthma- Rhinitis(symptomatology)
Comparisons between the moments T0 and T12

Figure 3
Bronchitis – dyspnea (intensity)
Comparisons between the moments T0 and T12
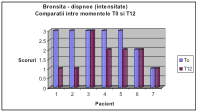
Figure 4
Thus, we applied the non-parametric test Wilcoxon (the rank sign) to each lot (both with asthma and bronchitis) and we obtained the following results (table 3 and 4):
| Bronchitis
|
p-level |
Significance |
| M* |
0.138 |
NS |
| E* |
0.0678 |
NS |
| D* |
0.0179 |
S |
| W* |
0.9 |
NS |
| B2* |
0.3613 |
NS |
| S* |
0.1088 |
NS |
| global |
< 0.001 |
ES |
*T,M,E,.. represent abbreviation of the symptoms in table I
Table 3
| Asthma
|
p-level |
Significance |
| T* |
0.0499 |
S |
| M* |
0.0076 |
FS |
| E* |
0.0277 |
S |
| W* |
0.0431 |
S |
| D* |
0.9 |
NS |
| B2* |
0.2249 |
NS |
| R* |
0.0499 |
S |
| global |
< 0.001 |
ES |
*T,M,E,.. represent abbreviation…
Table 4
When we compared the scores of the study lots to the scores of the control lots with the one of the control one, we applied the non-parametric test Mann-Whitney, the following results being obtained (table 5 and 6).
| Astm
|
p-level |
Semnific. |
| T* |
0.0067 |
FS |
| M* |
0.3285 |
NS |
| E* |
0.5098 |
NS |
| W* |
0.6347 |
NS |
| D* |
0.6569 |
NS |
| B2* |
0.4082 |
NS |
| R* |
0.2376 |
NS |
| global |
0.0022 |
FS |
*T,M,E,.. represent abbreviation of the symptoms in table I
Table 6
| Bronşită
|
p-level |
Semnific. |
| M* |
0.138 |
NS |
| E* |
0.0678 |
NS |
| D* |
0.0179 |
S |
| W* |
0.9 |
NS |
| B2* |
0.3613 |
NS |
| S* |
0.1088 |
NS |
| global |
< 0.001 |
ES |
*T,M,E,.. represent abbreviations of the symptoms
Table 5
The fact that the global estimation of all symptoms in those two lots (study and control) has a significance much different from the significances obtained per each symptom is due to the insufficient number of cases.
The examination of the pulmonary function both at asthma and bronchitis suffering patients has not indicated a significant improvement: the asthmatic patients showed a FEV1 of : 74.54± 4.35% at T0 and 77,12±6,13%at T 12 m and the bronchitis suffering patients showed 76,18±12,14% at T0 and 74,45±4,67 at T12m . Considering the digit 2 as an acceptable number of recurrences/year, both for the lot with asthma and the lot with bronchitis, graphically underlined in the figures 5 and 6, we compared using Ztest of significance, the ratio of 4 out of 10 persons ( asthma, Lot I of study)with 8 out of 9 persons ( asthma, Lot II of control) and we obtained the value p=0.0414(significant differences)analogous, ratio 1 out of 7 patients(bronchitis, lot I of study) and 3 out of 4 patients (bronchitis, lot II of control) and we obtained the values p= 0,0749( significant differences at the limit, having in view the small number of investigated subjects).

Figura 5

Figura 6
Answering to a simple questionnaire relating to the estimation of the living quality, the most patients (67%) alleged an improvement, 30% did not feel any improvement, and 1 patient (3%) claimed a worsening.
Discussions
The salt and water transport across alveolar and distal airway epithelia is under elucidation, its alteration being involved in the generation of some severe diseases: cystic fibrosis, pseudoaldosteronism. The studies performed at molecular and cellular level, as well as on animals demonstrated that the fluid reabsorption from the distal airways of the lung is a phenomenon directed by the active transport of sodium. Several studies in-vivo, in-situ or on an isolated lung identified catecolamine dependent mechanisms, as well as other independent mechanisms which modulate the fluid transport by activating the Na, K-ATPazeor by increasing the apical up-take due to the opening of “some channels for water” also called aquaporines,of 30kDa). (Matthay M Folkesson H., - 1996). Therefore, the interventions intended to modify the osmolarity of the pericilliary bronchial fluid can have significant consequences on local homeostasis and pulmonary function.
Anderson SD, Spring J (1997) in a rigorous study, compared the effect of wet aerosol of NaCl 4.5% with the effect of the aerosol inhalation as a dry powder, in variable quantities (5,10,20 or 40 mg). The results were overlapped and reproductible, concluding that the dry powder can replace the wet aerosols of NaCl(solution) in the tests made to provoke or estimate the bronchial hyperreactivity. The penetrability could be first determined by the magnitude of the bronchial constriction at the time of inhalation(Laube B, Swift D - 1986) and, further, by the aerosol tonicity Phipps P, Gonda - 1994), as the hypotonic solutions penetrate deeper.
Numerous studies attested the idea that the hypertonic aerosols (4.5%) of NaCl cause bronchial hyperreactivity, reason why these are used in clinic for the provoking tests, next to histamine, methacholine, according to some having higher specificity and predicting value than the first ones. But, the isotonic aerosols have not noxious effects.
However, the non-isotonic concentrations of non-isotonic aerosols, either hypo- or hyper-, as these modify the osmolarity of bronchial pericilliary fluid, can induce a crisis of bronchial spasms(Basir R – 1995, Smith C 1987); there are evidences that the modification of the osmolairty of the fluid in the airways causes a release of some mediators from the bronchial inflammatory cells.
On the other hand, speleotherapy offers a natural example of a beneficial impact on most of the chronic pulmonary disease. The speleotherapy implies the using of the underground environment ( especially of the salt mines) in the treatment of the chronic obstructive pulmonary diseases. Little known in U.S.A. and U.K., this procedure is largely used in central and Eastern Europe.
However, in the Western Europe authors, like Sadaul P (1981) mention it as having beneficial effects to over 90% of asthmatic persons who resorted to this therapeutical alternative, too.
Chernova O, Matiushina S (1996) showed the capacity of speleotherapy in salt mines to diminish the microbial contamination of the upper air ways (especially with staphylococcus), for children with respiratory allergy. The bactericide capacity could be explained by the complex immuno-modulating effects this procedure induces: the increase of the number and the activation of T lymphocytes, the normalization of the number of B-lymphocytes, the increase of the IgA level
(Simionka I, Chonka I – 1989). Abdullaev A and Gadzhiev K (1993) demonstrated the efficiency of speleotherapy in diminishing the obstructive symptom on 216 children with atopic asthma.
Further, Gorbenko P şi Adamova I (1996) on 18 patients with bronchial asthma, attested the effect of bronchial hyperactivity lowering after the exposure to halotherapy. In the same period, Borisenko L şi Chervinskaia (1995),specified a concentration of NaCl ions between 1 – 5mg /m3 spread in the air as dry powder as having a therapeutical value.
Given these considerations the method proposed by us is thought as an artificial micro-speleotherapy.
We achieved a continuous air ionization with dry powder of NaCl, which we supposed spread for 8-12 hours in a large environment, as a room could be, that would never get to a hypertonic concentration, on a contrary.
However, there is a limit as we do not know the quantity of ions delivered per minute in the environment and /or the concentration/m3.
In the future, the possibility to quantify these ions would offer the certitude that concentrations of non-istonic aerosols are avoided.
Only one patient, an asthmatic subject, claimed a worsening of the general condition after the air was ionized with Salin ; we do not know if that was just a subjective impression or a rise of an atmospheric concentration of the Na which increases HRB, as he refused the test of bronchial provoking with methacholine.
Though the pulmonary function does not appear modified, the improvement of symptoms like the sensation of humid neck with claims of impurities / stagnant secretions on pharynx-traehea(the increase of nasal permeability), sometimes with the snoring elimination, a reduced coughing , a lowering of sputum volume and a easiness to remove it, the smell improvement (2/5) gave the patients more quiet nights with an attenuated symtomatology in the morning, with more seldom and less discomfortable rhinitis phenomena, all these being reflected in the improvement of the living quality.
Conclusions
As an adjuvant treatment, the forced ionization of in-door air, though it does not improve significantly the pulmonary function, improves, however the quality of the patients` life and reduces the rate of annual hospitalizations. It is worth being mentioned the method advantages: has no risk, is cheap and adapted to the living space.
Bibliography
ANDERSON SD., SPRING J., MOORE B. and colab., The effect of inhaling a dry powder of sodium chloride on the airways of asthmatic subjects, Eur. Respir. J. 1997 Nov; 10(11): 2465-73 Related articles, Books. ABDULAEV AA., GADZHIEV KM., EIUBOVA AA., The efficacy of speleotherapy in salt mines in children with bronchial asthma based on the data from immediate and late observations, Vopr. Kurortol. Fizioter. Lech. Fiy. Kult. 1993 Sept-oct: (5): 25-8; Barry P, Fouroux B, Pedersen S et al., Nebulizers in childhood., Eur Respir Rev., 2000; 10:76, 527-535. BASIR R., LEHRMAN SG., DE LORENZO LJ.AND COLAB., Lack of significant bronchial reactivity to inhaled normal saline in subjects with methacoline challenge test, J Asthma 1995; 32 (1): 63-7; Boe J, Dennis J, O’Driscoll B., ERS nebulizers guidlines: clinical aspects., Eur Respir Rev 2000, 10:76, 495-496. BORISHENKO LV., CHERVINSKAIA AV., STEPANOVA NG., The use of halotheraphy for the rehabilitation of patients with acute bronchitis and a protracted and recurrent course, Vopr. Kurortol. Fizioter. Lech. Fiz. Kult. 1995 Jan-Feb.; (1) : 11-5; CHERNOVA OP., MATIUSHINA SB., VOLIANIK MN. and colab., The dynamics of the persistence characteristics of staphylococci under the action of the microclimate of a speleotherapy mine, Zh. Mikrobiol Immunobiol. 1996 May-Jun: (3): 78-80; GORBENKO PP., ADAMOVA IV., SINITSYNA TM., Bronchial hyperreactivity to inhalation of hypo- and hyperosmolar aerosols and its correction by halotherapy, Ter. Arkh. 1996; 68(8): 24-8. Juniper EF., O’Byrne, Guyatt G et al, Development and validation of a questionnaire to mesure asthma control., Eur Respir J 1999; 14: 902-907.Juniper EF., O’Byrne, Ferrie P et al., Measuring asthma control: clinic questionnaire or daily diary ? Am J Respir Crit Care Med 2000; 163:1330-1334. Kugelman A, Durand M, Garg M et al., Pulmonary effect of inhaled furosemide in ventilated infants with severe bronchopulmonary dysplasia., Pediatrics., 199799., 71-75. LAUBE BL., SWIFT DL., WAGNER HN. Jr. and colab., The effect of bronchial obstruction on central airway deposition of a saline aerosol in patients with asthma, Am. Rev. Respir. Dis. 1986 May, 133 (5): 740-3. MATHAY MA, FOLKESSON HG, VERKMAN AS., Salt and water transport across alveolar and distal airway epithelia in the adult lung, Am. J. Physiol. 1996 Apr. 270 (4 Pt 1): L487-503; PHIPPS PR., GONDA I., ANDERSON SD.and colab., Regional deposition of saline aerosols of different tonicities in normal and asthmatic subjects, Eur. Respir. J. 1994, Aug.; 7(8): 1474-82; RIEDLER J., READE T., ROBERTSON CF., Repeatability of response to hypertonic saline aerosol in children with mild to severe asthma, Pediatr. Pulmonol. 1994 nov, 18(5) : 330-6. SADOUL P., Maladies chroniques des bronches., edite par PIL., pg., 195-196., 1982. SIMIONKA IUM., CHONKA IAV, POP IL., Effect of the microclimate of salt mines on T- and B- lymphocyte function in bronchial asthma patients, Vrach Delo 1989 Mar.; (3): 57-9;








